Everyone's launching a DTP model right now. And most of them are going to be surprised by what they signed up for.
Selling direct to patients sounds simple - cut out the middleman, own the relationship. But the moment you ship product directly to a patient's door, you're no longer just a drug manufacturer. You're responsible for getting it there, answering questions when something goes wrong, and navigating a whole set of rules your legal and supply chain teams haven't had to think about before.
TrumpRx accelerated the timeline, but the risks were always there. Here's the map.
Most pharma commercial teams are designed to sell to wholesalers, distributors, and specialty pharmacies - not to individual patients. When you go direct, you inherit responsibilities that those intermediaries used to carry: unit-level inventory tracking, customer-facing returns processes, state-by-state sales tax collection, and the kind of product recall infrastructure that works at the individual address level, not the pallet level.
That's a different business. And most DTP programs are being designed as if it isn't.
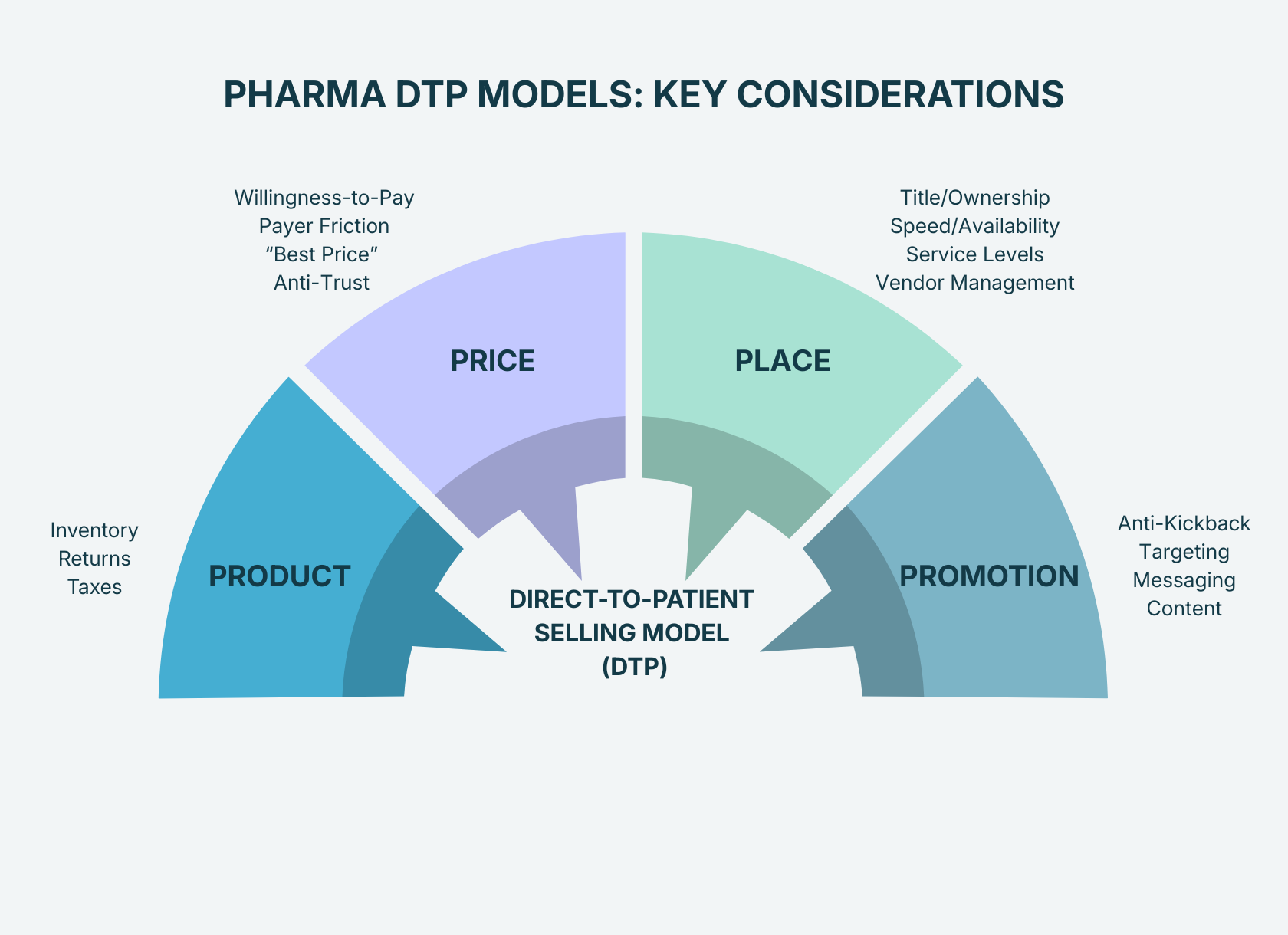
The risks map cleanly onto the 4 Ps of marketing: Product, Price, Place, and Promotion. Each one carries a distinct category of exposure. Most pharma teams see one or two of them clearly and miss the rest entirely.
When you ship directly to patients, you're no longer moving pallets. You're moving individual units to thousands of addresses - which means you suddenly have the responsibilities of a retailer. You become accountable for unit-level inventory, product recalls, and patient-facing returns. Whether you decide to hire third-party logistics partners (3PL) or handle them yourself, make sure you consider each aspect and leverage our downloadable checklist as guidance.
DTP turns pricing into a patient decision-making moment - and simultaneously raises the stakes with payers and government price reporting requirements. Your DTP price doesn't exist in a vacuum: it interacts with contracted payer rates, Best Price calculations, and Medicaid rebate obligations. It effectively becomes your "manufacturer suggested retail price" and provides price transparency to every stakeholder involved.
Place is your business model - it determines how patients pay for and receive the product. Depending on how accessible your product needs to be, you could go with a centralized (single mail-order pharmacy) or a distributed model (multiple pharmacies). Remember that the moment you own the distribution channel, you own the operational risk that comes with it, so don't undervalue the operational excellence required to make a DTP program work.
This is the most legally sensitive area. The Anti-Kickback Statute (AKS) is designed to prevent financial incentives from improperly influencing medical decisions - and violation is a criminal offense, not just a compliance slap on the wrist. Plus, you're risking the rest of your business from being excluded from federal programs like Medicare.
DTP isn't just a new channel. It's a bundle of product movement, financial flows, and patient engagement that can either feel effortless - or become a compliance and operational headache. The difference is almost always in how carefully the program was designed before launch.
Most of these risks are fixable. But they're much easier to fix before you've signed contracts, set prices, and shipped your first order.
Download the free resource to complete a 4P risk review of your DTP program or reach out to speak to one of our experts.
.png)
